New edition
Tumour metastasis
Cancer is usually not curable when metastases have formed in the body. Metastases are often resistant to drugs that have successfully eliminated the primary tumour. The basic features of the complex process of metastasis are now known, but many details still remain elusive. Intensive research activities are focusing on new therapeutic concepts aimed at developing effective anti-metastatic therapies.
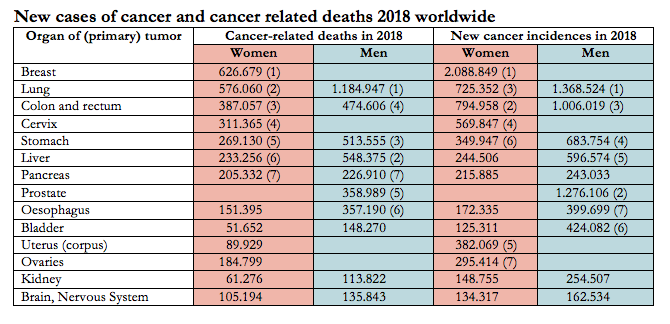 There is no reliable statistical information on the degree of metastasis of the tumours; but we do know that most cancer-related deaths are caused by metastases. The numbers in brackets indicate the order of frequency in each category. Source: Global Cancer Statistics 2018 (GLOBOCAN estimates) in CA: Cancer J. Clin. 2018; 68:394-424
© BIOPRO Baden-Württemberg GmbH
There is no reliable statistical information on the degree of metastasis of the tumours; but we do know that most cancer-related deaths are caused by metastases. The numbers in brackets indicate the order of frequency in each category. Source: Global Cancer Statistics 2018 (GLOBOCAN estimates) in CA: Cancer J. Clin. 2018; 68:394-424
© BIOPRO Baden-Württemberg GmbH
Metastases are responsible for 90 percent of the 220,000 cancer deaths in Germany every year (and around 9.6 million globally). Metastases are secondary tumours that detach from the primary tumour and colonise remote parts of the body. The likelihood of metastases forming varies dramatically between cancers, as shown in the figures for cancer diagnosis and deaths in the table below. Where the number of deaths is similar to the number of newly diagnosed patients, the tumours in question are particularly malignant and metastatic. Metastases often occur long after the primary tumour has been eliminated by effective therapy. Metastases are difficult to treat because they are often very different from the cancer cells of the original tumour. For example, metastases can be resistant to chemotherapeutic drugs that have successfully eliminated the primary tumour. Despite its enormous medical importance, the highly complex process of metastasis is still not understood in detail. However, the good news is that within the last decade or so the basic features have been elucidated by global cancer researchers.
The multistep process of metastasis
While it was previously posited that only large, advanced primary tumours form metastases, recent evidence suggests that cancer cells can disseminate and reach remote sites from very small, diagnostically barely detectable primary tumours. Metastasis is a multi-step cascade, beginning with what is known as local invasion, i.e. individual or small aggregates of tumour cells breaking through the barriers around a primary tumour (e.g. an epithelium with basal lamina) and invading the connective tissue surrounding the tumour. In a second step, referred to as intravasation, the tumour cells cross the endothelial barrier and enter a blood or lymph vessel. In some cases, for example ovarian cancer, metastasis can occur directly within the body cavity. Lymphogenous spread (via a lymph vessel) results primarily in metastases in nearby lymph nodes, while distant metastases arise from cells that spread haematogenously (via the bloodstream). This article will exclusively focus on the latter, and not on tumour cells that lodge in lymph nodes.
Circulating tumour cells (CTC) are found in metastatic breast and lung cancers as well as in prostate and colorectal cancers. However, no correlation has been found between the number of CTCs and the extent of metastasis. According to information provided by Michael Baumann, Chairman and Scientific Director of the German Cancer Research Center (DKFZ) in Heidelberg, only a very small proportion (one in around 10,000 cells) of CTCs is able to form metastases. This finding corresponds with the finding that the blood of advanced breast cancer patients contains a unique population of CTCs called metastasis-initiating cells (MICs). MICs possess stem-cell characteristics and form metastases more easily than other CTCs. Heidelberg stem cell researchers led by Andreas Trumpp from the DKFZ showed in an animal model that such MICs can actually give rise to bone metastases.
It is assumed that most tumour cells that circulate in the blood are eliminated by the body's own immune cells as they patrol the bloodstream. However, some tumour cells can evade the immune cells via platelets that adhere to their surface. Occasionally, these tumour cells also form small, platelet-clad cell aggregates that are even better protected against immune attacks. Many tumour cells that circulate in the blood are arrested in the lungs; tumour cells in the blood of the gastrointestinal tract are usually arrested in the liver. However, some tumour cells or small tumour cell aggregates also manage to spread through the bloodstream to other organs. In the final step, known as extravasation, the tumour cells can then penetrate the endothelium of the blood capillaries and colonise the surrounding tissue. The Heidelberg oncologist and vascular expert Andreas Fischer proved that cancer cells and endothelial cells actively interact with each other, for example through the formation of specific docking proteins. It has already been possible to successfully block this process using antibodies – a promising approach for the treatment of metastatic cancer.
 Prof. Dr. med. Frank Winkler, Head of the Experimental Neurooncology Research Group and Consultant, Department of Neurology at Heidelberg University Hospital.
© Medical Centre, Heidelberg University Hospital
Prof. Dr. med. Frank Winkler, Head of the Experimental Neurooncology Research Group and Consultant, Department of Neurology at Heidelberg University Hospital.
© Medical Centre, Heidelberg University Hospital
Distant metastases can arise in many organs of the body, but different cancers prefer different organs. As far back as 130 years ago, the British surgeon Stephen Paget postulated that cancer cells, like seeds, must find “fertile soil” to grow. Cancer cells need specific growth factors and receptors so that they can be taken up and survive in the target organ. Exosomes, which are small membrane vesicles that contain signal molecules and messengers and are able to segregate from the tumour cells, appear to play an important role in this process. The interaction between tumour cells and the connective tissue and endothelial cells leads to the formation of a "pre-metastatic niche", in which the cells can hide and survive over long periods of time. For example, metastatic melanoma cells, lung cancer cells and cells of certain forms of breast cancer prefer to colonise the brain, "although,” as the Heidelberg neuro-oncologist Frank Winkler explains, “it is not very easy for cancer cells to get there". He has shown in the mouse model that these tumour cells adhere to the outside of the capillary endothelial cells after extravasation and, along with certain brain cells, form a "vascular niche" in which they can remain inactive for a long time. How these "sleepers" manage to become dreaded brain metastases, usually many years later, is one of the questions being asked in a cooperative project entitled “Preventive strategies for brain metastasis”. The project, which is funded by German Cancer Aid and led by Professor Winkler, involves nine research groups from across Germany, and one of its goals is to test commercially available drugs for their ability to cross the blood-brain barrier and influence the interactions between tumour cells and the brain.
Precision oncology
Cells hiding in the “vascular niche” are usually resistant to chemotherapy or radiotherapy, two treatments which can destroy active, dividing cancer cells, and successfully suppress primary tumour growth. A strategy for combating metastatic tumours, which has only been shown to be effective for blood cancers, is aimed at awakening dormant tumour cells, triggering cell division and making them vulnerable to chemotherapy with cytostatic drugs.
In the target organ, tumour cells must fulfil various conditions to be able to grow into secondary tumours, i.e. growth factors that lead to neovascularisation (neoangiogenesis). Growing tumours that have reached one millimetre in diameter require blood vessels that supply them with oxygen and nutrients. Angiogenesis inhibitors, used to suppress vascularisation and starve the tumour, have long been part of the treatment repertoire in oncology.
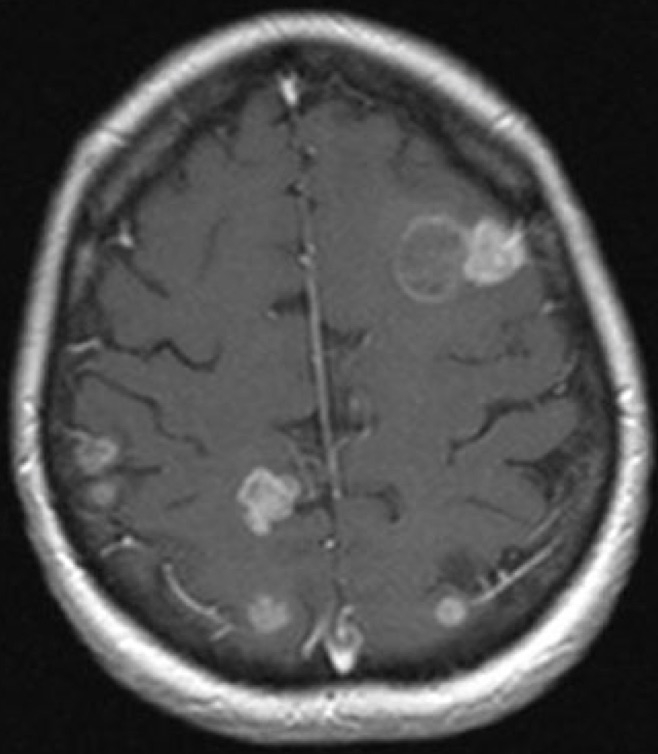 Magnetic resonance image of a patient’s brain metastases.
© Heidelberg University Hospital
Magnetic resonance image of a patient’s brain metastases.
© Heidelberg University Hospital
The growth of life-threatening metastases is the result of a series of mutations and a selection process that enables individual cancer cells to escape the various barriers and defence mechanisms of the body and thrive in an alien biophysical environment with different metabolic conditions. For example, it has been shown that metastatic breast cancer and prostate cancer cells that had colonised bone tissue were able to activate genes that bone cells also activated. As a result of rigorous selection, metastatic cancer cells are often resistant to drugs that have been successfully used to treat the primary tumour. However, genetic changes differ from patient to patient. The genomes and expression profiles of each tumour and its metastases have to be analysed in order to tailor therapies to individual patient requirements.
"Personalised/precision oncology" of this kind is not yet standard clinical practice, but this "genomically informed medicine" is being explored, for example, in a study on metastatic breast cancer at the National Center for Tumor Diseases (NCT) and the DKFZ involving “omics profiling” (genomics, transcriptomics, etc.). Omics profiling can also help identify the origin of metastases by comparing tumour tissue to different body tissues in cases when the primary tumour is unknown. This is referred to as a "cancer of unknown primary" (CUP). At present, CUPs generally have a poor prognosis, and are treated with platinum-based chemotherapy. However, a new immunotherapy approach using so-called immune checkpoint inhibitors promises better results. Antibodies, which block signalling proteins on immune cells and as a result activate the body’s own immune defence, have already led to spectacular results in the treatment of metastatic melanomas.
The development of this new class of drugs, for which James P. Allison and Tasuku Honjo received the Nobel Prize in Physiology and Medicine in 2018, is an excellent example of how basic oncology research can even improve the treatment of advanced metastatic tumours. Michael Baumann highlighted these successes at the opening of the 1st German Cancer Research Congress, which took place in Heidelberg in February 2019, marking the start of the German Government's proclaimed "National Decade Against Cancer". Baumann, who is also co-chair of the National Decade strategy circle, contradicted the Federal Minister of Health who stated in comments to the newspaper "Rheinische Post" (which were later attenuated) that "we might be able to defeat cancer in 10 to 20 years’ time". Baumann said that we will most likely witness a 20 percent increase in cancer cases by 2030 alone. Cancer prevention and the early detection of tumours aimed at complete tumour destruction before the onset of metastasis must therefore become a priority, and the National Decade against Cancer is setting out to “stop metastasis at source”. As an expert involved in the initiative said, this goal can only be achieved if everyone works together in the fight against tumours.