Cancer therapy and cancer diagnostics
Thanks to improved diagnostics and therapy, today’s cancer patients can live considerably longer than patients several years ago. Nevertheless, some cancers, especially the strongly metastatic ones, are difficult to treat. Therapies targeting immune cells or cancer stem cells could potentially improve the current situation. The early detection and classification of tumours is crucial for the successful treatment of the disease, and molecular diagnosis involving biomarkers and genome analyses are important for personalising cancer therapy.
 The radiation cannon in the gantry of the Heidelberg Ion-Beam Therapy Centre (HIT). This is the biggest medical device for the treatment of cancer in the world.
© HIT
The radiation cannon in the gantry of the Heidelberg Ion-Beam Therapy Centre (HIT). This is the biggest medical device for the treatment of cancer in the world.
© HIT
EUROCARE-5, the largest European study on cancer survival, shows that in general, patients in Germany survive much longer after a cancer diagnosis than they did a few years ago. The researchers noted the highest increases for rectal cancer, non-Hodgkin lymphomas as well as for childhood leukaemias. This may be due to progress in chemo- and radiotherapies, which today can be better adjusted to the characteristics of a tumour. The high precision achieved by combined imaging methods and novel radiation equipment enables promising treatment of cancers that were unresponsive to treatment in the past.
Survival rates have improved for almost all body systems affected by cancer and are a key measure of the progress in and effectiveness of healthcare systems, especially as far as diagnosis is concerned. Early detection of cancer greatly increases the chances of successful treatment. Major problems are caused by tumours that grow deep inside body organs and therefore cannot be seen during an examination, forming metastases that are difficult to detect and treat. Oncological research is specifically focused on the discovery and development of reliable biomarkers to improve the early detection of such tumours and their metastases.
Gatekeeper diagnostics and personalised therapies
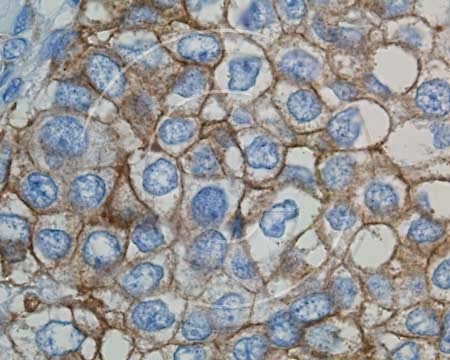 Immunohistochemical detection of Her2/neu (epidermal growth factor 2 receptor) in breast cancer cells.
© Department of Pathology, Vechta
Immunohistochemical detection of Her2/neu (epidermal growth factor 2 receptor) in breast cancer cells.
© Department of Pathology, Vechta
Extensive genetic variation exists not only between tumours but also within individual tumours. Therefore there are great expectations for individualised or personalised therapies, i.e. therapies tailored to the requirements of individuals (or more realistically: individual groups of people). The effect of state-of-the-art biopharmaceuticals that target specific molecules has been shown to differ in relation to the genetic characteristics of the tumour cells.
Tumours can only be effectively treated if they have been correctly classified. New diagnostic and detection methods (especially molecular biomarkers, genetic and genomic analyses) have become so-called gatekeepers for biopharmaceuticals that are safe and effective treatments for patient populations with a specific genetic profile, and therefore help minimise harmful side effects. Herceptin (trastuzumab) is one of the most common examples of personalised medicine. Trastuzumab is a recombinant antibody that interferes with the Her2/neu receptor. It is used to treat breast cancer patients who overexpress the receptor. Around 20% of women with breast cancer are Her2/neu positive.
Tamoxifen, a drug that is used for the treatment of ER+ (oestrogen receptor positive) breast cancer, is another example from which only a specific patient group benefits. Only women with an oestrogen receptor benefit from tamoxifen treatment. Patients with colorectal cancer are recommended to undergo routine KRAS screening as the oncogene is often mutated in colorectal cancers. Patients with mutated KRAS are not responsive to EGF (epidermal growth factor) inhibitors. Moreover, the treatment of chronic myeloid leukaemia with Glivec (imatinib) is only successful in patients with a specific chromosomal translocation (BCR-ABL).
New methods enable the early diagnosis of cancer
Criticism that abounded only a few years ago has been silenced. In 2010, even prominent figures such as Nobel laureate Harold Varmus still believed that genomics and related disciplines contributed very little to medical progress. However, it has since been shown that molecular analyses of tumour DNA provide information relating to which therapy is likely to have the greatest chance of success. The German Cancer Research Center in Heidelberg and other famous cancer institutes around the world have therefore started carrying out routine whole-genome analyses in patients with specific tumours. The number of individualised anti-cancer drugs is expected to increase considerably in future and information about genome sections that are not currently considered as drug targets will also gain in importance.
Other molecular tumour markers are also becoming more important for the diagnosis of cancer, including chromosomal damage associated with leukaemia and epigenetic alterations associated with colon cancer. One particularly interesting iron in the fire is the development of blood tests ("liquid biopsy tests") with which tumour genes or tumour-specific microRNA patterns can be detected. The tests are still in the experimental stage, but the researchers hope that blood samples will soon play a significant role in the early diagnosis of cancers that can only currently be detected at an advanced stage and are no longer susceptible to treatment. This includes lung, pancreatic and liver cancer, all of which are typically diagnosed at a late stage because they do not give rise to symptoms until it is too late. At present, 85 to 90 percent of all lung, pancreatic and liver cancer patients die within five years of diagnosis.
The study also showed that for cancers of the prostate, breast, thyroid and testicles, melanomas and Hodgkin lymphomas, five-year survival after diagnosis is over 80 percent. This is due to the improved detection of early cancers, progress in surgical and radiological therapies and improved medical therapy.
Immunotherapy and cancer stem cells
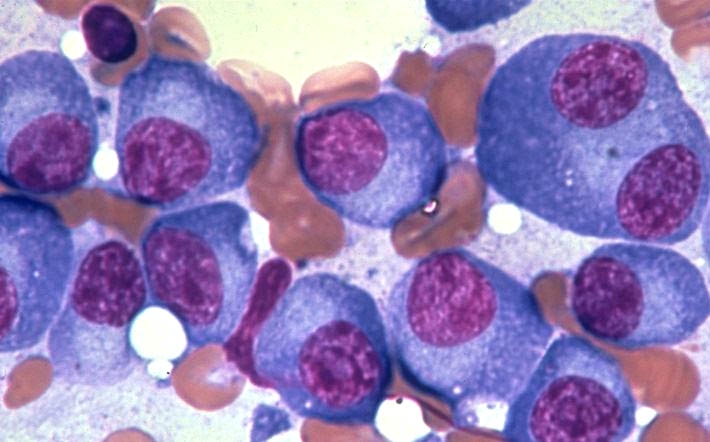 In multiple myeloma, a cancer of the bone marrow, abnormal plasma cells accumulate.
© Heidelberg University Hospital
In multiple myeloma, a cancer of the bone marrow, abnormal plasma cells accumulate.
© Heidelberg University Hospital
The malignancy of cancer is mainly due to its ability to evade the attack of the body’s immune cells (T lymphocytes, NK cells) that are able to detect and destroy tumour cells. Many research groups are therefore working on therapeutic approaches that have the potential to activate the immune system against cancer cells. These approaches also need to take into account the patient’s genetic and physiological constitution. In combination with efficient diagnostic procedures, the personalised immunotherapy of cancer is a promising concept on our way towards the successful treatment and cure of cancer. In 2013, studies reporting on the development of T lymphocytes that carried surface receptors required for the recognition of cancer cells from induced pluripotent stem cells (iPS) attracted worldwide attention. Little is yet known as to whether such laboratory results can be used for the successful treatment of human cancer.
Initial practical success has been achieved with approaches targeting cancer stem cells. Such cancer stem cells are unresponsive to standard chemotherapeutic drugs and have since been described for many cancers. These stem cells are cancer cells that are responsible for the recurrence of a tumour years after successful removal and they can also give rise to metastases. They can be identified with specific biomarkers, including the growth factor receptor MET that promotes the formation of blood vessels in tumours (angiogenesis). Drugs that are able to inhibit MET are currently in clinical development.
EJ – 10.03.2014
© BIOPRO Baden-Württemberg GmbH